


 Sign Out
Sign Out



Pharmacology: Pharmacodynamics: Mechanism of action: VaxigripTetra provides active immunisation against four influenza virus strains (two A subtypes and two B types) contained in the vaccine.
VaxigripTetra induces humoral antibodies against the haemagglutinins within 2 to 3 weeks. These antibodies neutralise influenza viruses.
Specific levels of haemagglutination-inhibition (HAI) antibody titre post-vaccination with inactivated influenza virus vaccines have not been correlated with protection from influenza illness but the HAI antibody titres have been used as a measure of vaccine activity. In some human challenge studies, HAI antibody titres of ≥1:40 have been associated with protection from influenza illness in up to 50% of subjects.
Since influenza viruses constantly evolve, the virus strains selected in the vaccine are reviewed annually by the WHO.
Annual revaccination with VaxigripTetra has not been studied. However, based on clinical experience with the trivalent vaccine, annual influenza vaccination is recommended given the duration of immunity provided by the vaccine and because circulating strains of influenza virus change from year to year.
Efficacy of VaxigripTetra: Paediatric population: Children from 6 to 35 months of age (active immunisation): A randomized placebo controlled study was conducted in 4 regions (Africa, Asia, Latina America and Europe) over 4 influenza seasons, in more than 5,400 children from 6 to 35 months of age who received two doses (0.5 mL) of VaxigripTetra (N=2,722), or placebo (N=2,717) 28 days apart to assess VaxigripTetra efficacy for the prevention of laboratory-confirmed influenza illness caused by any strain A and/or B and caused by vaccine similar strains (as determined by sequencing).
Laboratory-confirmed influenza illness was defined as influenza like-illness (ILI) [occurrence of fever ≥ 38°C (that lasts at least 24 hours) concurrently with at least one of the following symptoms: cough, nasal congestion, rhinorrhoea, pharyngitis, otitis, vomiting, or diarrhoea], laboratory-confirmed by reverse transcriptase polymerase chain reaction (RT-PCR) and/or viral culture. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn addition, a predefined complementary analysis showed VaxigripTetra prevented 56.6% (95% CI: 37.0; 70.5) of severe laboratory-confirmed influenza illnesses due to any strain, and 71.7% (95% CI: 43.7; 86.9) of severe laboratory-confirmed influenza illnesses due to vaccine similar strains.
Furthermore, subjects receiving VaxigripTetra were 59.2% (95% CI: 44.4; 70.4) less likely to experience a medically attended influenza illness than subjects receiving placebo.
Severe laboratory-confirmed influenza illnesses were defined as ILI laboratory-confirmed by RT-PCR and/or viral culture with at least one of the following items: fever > 39.5°C for subjects aged < 24 months or ≥ 39.0°C for subjects aged ≥ 24 months, and/or at least one significant ILI symptom which prevents daily activity (cough, nasal congestion, rhinorrhoea, pharyngitis, otitis, vomiting, diarrhoea), and/or one of the following events: acute otitis media, acute lower respiratory infection (pneumonia, bronchiolitis, bronchitis, croup), inpatient hospitalisation.
Children from 3 to 8 years of age (active immunisation): Based on immune responses observed in children from 3 to 8 years of age, the efficacy of VaxigripTetra in this population is expected to be at least similar to the efficacy observed in children from 6 to 35 months (see "Children from 6 to 35 months of age" as previously mentioned and "Immunogenicity of VaxigripTetra" as follows).
Infants less than 6 months of age born to women vaccinated during pregnancy (passive protection): Infants less than 6 months of age are at high risk of influenza, resulting in high rates of hospitalisation; however influenza vaccines are not indicated for active immunisation in this age group.
The efficacy in infants born to women who received a single 0.5 mL dose of VaxigripTetra during the second or third trimester of pregnancy has not been studied; however, the efficacy in infants born to women who received a single 0.5 mL dose of the trivalent inactivated influenza vaccine (Vaxigrip) during the second or third trimester of pregnancy has been demonstrated in clinical trials and can be extrapolated to VaxigripTetra.
The efficacy of the trivalent inactivated influenza vaccine (Vaxigrip) in infants born to women vaccinated during the first trimester of pregnancy has not been studied in these trials. If influenza vaccination is considered necessary during the first trimester of pregnancy, it should not be postponed (see Use in Pregnancy & Lactation).
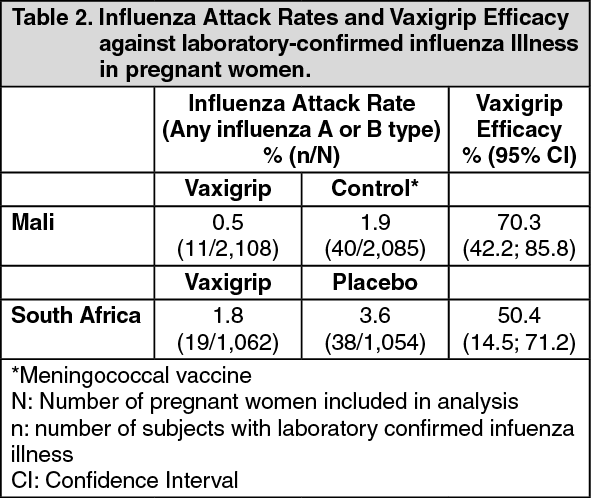
In randomised, controlled phase IV clinical studies conducted in Mali, Nepal and South Africa, approximately 5,000 pregnant women received Vaxigrip (trivalent influenza vaccine) and approximately 5,000 pregnant women received a placebo or control vaccine (quadrivalent meningococcal conjugate vaccine) during the second or third trimester of pregnancy. Vaccine efficacy against laboratory confirmed influenza illness in pregnant women was evaluated as a secondary endpoint in all three studies.
The studies conducted in Mali and South Africa demonstrated the efficacy of Vaxigrip for the prevention of influenza in pregnant women following vaccination during these trimesters of pregnancy (see Table 2). In the study conducted in Nepal, the efficacy of Vaxigrip for the prevention of influenza in pregnant women following vaccination during these trimesters of pregnancy was not demonstrated. (See Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn the same randomised, controlled, phase IV clinical studies conducted in Mali, Nepal and South Africa, 4,530 of the 4,898 (92%) infants born to women who received Vaxigrip (trivalent influenza vaccine) during the second or third trimester of pregnancy, and 4,532 of the 4,868 (93%) infants born to pregnant women who received a placebo or control vaccine (quadrivalent meningococcal conjugate vaccine) during the second or third trimester of pregnancy (see Table 3) were followed-up until approximately 6 months of age.
These studies confirmed the efficacy of Vaxigrip for the prevention of influenza in infants born to women vaccinated during these trimesters of pregnancy, from birth until approximately 6 months of age. Women in their first trimester of pregnancy were not included in these studies; the efficacy of Vaxigrip in infants born to women vaccinated during the first trimester of pregnancy could therefore not be evaluated. (See Table 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe efficacy data indicate a waning protection over time, after birth, of the infants born to women vaccinated during pregnancy.
In the trial conducted in South Africa, vaccine efficacy was higher in infants 8 weeks of age or younger (85.8% [95% CI: 38.3; 98.4]) and decreased over time; vaccine efficacy was 25.5% (95% CI: -67.9; 67.8) for infants from 8 to 16 weeks of age and 30.4% (95% CI: -154.9; 82.6) for infants from 16 to 24 weeks of age.
In the trial conducted in Mali, there is also a trend to higher efficacy of the trivalent inactivated influenza vaccine in infants during the first 4 months after birth, with lower efficacy within the 5th month and a marked fall during the 6th month where protection is no longer evident.
The prevention of influenza can only be expected if the infants are exposed to the strains included in the vaccine administered to the mother.
Immunogenicity of VaxigripTetra: Clinical studies performed in adults from 18 to 60 years of age, in elderly over 60 years of age, in children from 3 to 8 years of age and from 6 to 35 months assessed VaxigripTetra immune response for HAI Geometric mean antibody titre (GMT) at Day 21 (for adults) and at Day 28 (for children), HAI seroconversion rate (4-fold rise in reciprocal titre or change from undetectable [< 10] to a reciprocal titre of ≥ 40), and HAI GMTR (post-/pre-vaccination titres).
One clinical study performed in adults from 18 to 60 years of age and in children from 9 to 17 years of age described the immune response of VaxigripTetra for HAI antibody GMT at Day 21. Another clinical study performed in children from 9 to 17 years of age described the immune response of VaxigripTetra.
One clinical study performed in pregnant women described the immune response of VaxigripTetra for HAI GMT at Day 21, HAI seroconversion rate, and HAI GMTR, after one dose administered during the second or third trimester of pregnancy. In this study, the transplacental transfer was evaluated using HAI GMTs of maternal blood, of cord blood and the ratio of cord blood/maternal blood, at delivery.
VaxigripTetra induced a significant immune response against the 4 influenza strains contained in the vaccine.
Adults and elderly: A total of 832 adults from 18 to 60 years of age and 831 elderly over 60 years of age were assessed in terms of immune response after one dose of VaxigripTetra.
Immunogenicity results are presented in the tables as follows: (See Table 4).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePregnant women and transplacental transfer: A total of 230 pregnant women received VaxigripTetra during the second or third trimester of pregnancy (from 20 to 32 weeks of pregnancy).
Immunogenicity results by HAI method, in pregnant women 21 days after vaccination with VaxigripTetra are presented in Table 5. (See Table 5.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageImmunogenicity descriptive assessment by HAI method, at delivery, in blood sample of mother (BL03M) and in cord blood sample (BL03B) and of the transplacental transfer (BL03B/BL03M) are presented in Table 6. (See Table 6.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAt delivery, the higher level of antibodies in the cord sample compared to the maternal blood sample is consistent with transplacental antibody transfer from mother to the foetus following vaccination of women with VaxigripTetra during the second or third trimester of pregnancy.
These data are consistent with the passive protection demonstrated in infants from birth to approximately 6 months of age following vaccination of women during the second or third trimester of pregnancy with Vaxigrip in studies conducted in Mali, Nepal, and South Africa (see subsection Efficacy of VaxigripTetra).
Paediatric population: Children from 9 to 17 years of age: In a total of 429 children from 9 to 17 years of age who received one dose of VaxigripTetra, the immune response against the 4 strains contained in the vaccine was similar to the immune response induced in adults from 18 to 60 years of age.
Children from 6 months to 8 years of age: A total of 863 children from 3 to 8 years of age received either one or two doses of VaxigripTetra depending on their previous influenza vaccination history. Children who received a one- or two-dose schedule of VaxigripTetra presented a similar immune response following the last dose of each schedule.
In addition to the VaxigripTetra efficacy, the immunogenicity of two 0.5 mL doses of VaxigripTetra was assessed 28 days after the last injection of VaxigripTetra by HAI method in 341 children from 6 to 35 months of age.
Immunogenicity results are presented in the table as follows: (See Table 7.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThese immunogenicity data provide supportive information in addition to vaccine efficacy data available in this population (see Efficacy of VaxigripTetra as previously mentioned).
Pharmacokinetics: Not applicable.
Toxicology: Preclinical safety data: Non-clinical data revealed no special hazard for humans based on conventional studies of repeat dose and local toxicity, reproductive and developmental toxicity and safety pharmacology studies.